By William B. Trattler, MD
Advances in intraocular lens (IOL) design, power calculation formulas, and surgical technologies are enabling the ability of cataract surgeons to achieve excellent visual and refractive outcomes. Dry eye disease (DED), however, presents a significant barrier to surgical success and patient satisfaction because it can reduce the reliability of preoperative measurements used for IOL power calculation and negatively impact visual quality after surgery.
These risks, together with evidence from multiple studies showing that preoperative treatment of DED improves surgical outcomes, underscore the importance of managing DED prior to cataract surgery. Recognizing that DED is highly prevalent in the cataract surgery patient population, frequently undiagnosed, and often asymptomatic highlights a need to make evaluation for DED a routine part of the preoperative workup for every cataract surgery patient.
In the PHACO (Prospective Health Assessment of Cataract Patients’ Ocular Surface) study published in 2017, we reported that only 25% of the 136 participating patients had a previous diagnosis of DED, while approximately 70% of our cohort reported minimal to no DED-related symptoms.1 On examination, however, nearly two-thirds of the enrolled patients had a tear break-up time (TBUT) of ≤5 seconds, over three-fourths had positive corneal staining, and half had positive central corneal staining.
In another study designed to characterize the prevalence of ocular surface dysfunction among patients presenting for cataract surgery evaluation, Gupta et al reported that 46% of patients reported no symptoms of DED based on questionnaire responses, but 85% of those individuals had at least 1 abnormal objective DED test result.2 Cochener et al evaluated meibomian gland dysfunction (MGD) in 180 patients presenting for cataract surgery and found that this leading cause of DED was present in 52% of participants, half of whom were asymptomatic.3
Straightforward Streamlined Screening
Findings from preoperative biometry often provide an initial clue that DED is present. In my practice, technicians use 3 different devices to obtain measurements: the IOLMaster 700 (Carl Zeiss Meditec), Pentacam (Oculus), and Cassini Ambient (Cassini Technologies). When I review the reports from these technologies, I check for consistency in the values for astigmatism magnitude and power. Significant lack of agreement strongly suggests the patient has visually significant DED that requires treatment followed by remeasurement to check for data reliability.
My clinical examination to detect visually significant DED focuses on assessments of tear volume, tear film stability, ocular surface damage, and lid margin disease. Findings that are indications for preoperative treatment of DED include presence of positive corneal fluorescein staining, low tear meniscus height, rapid TBUT, significant MGD, and Demodex blepharitis.
Point-of-care tests that analyze tear film osmolarity or the level of matrix metalloproteinase-9 (MMP-9) as a marker of inflammation can be helpful for detecting DED, although I do not include them in my preoperative workup. I also do not have patients complete any formal questionnaires that are designed to capture signs and symptoms of DED considering that some vision-related complaints are common for both DED and cataracts and, most importantly, the fact that DED is asymptomatic in so many cataract patients.
Rehabilitating the ocular surface
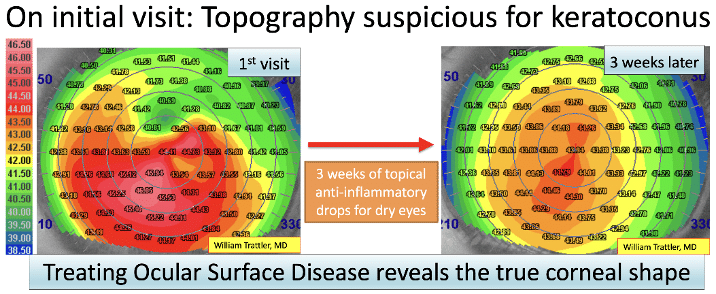
At the initial preoperative visit, I review surgical and IOL options with all patients and typically schedule surgery for 3 to 4 weeks later. Patients who require DED treatment are instructed to return in approximately 3 weeks for repeat examination that will confirm whether surgery can proceed on the date initially planned. In most cases, the ocular surface can be improved to get reliable preoperative biometry readings, allowing surgery to be done as scheduled (see Figure).
Treatment for inflammation is the mainstay of my approach to managing DED prior to cataract surgery. As recognized in the TFOS DEWS (Tear Film & Ocular Surface Society Dry Eye Workshop) II definition of DED, ocular surface inflammation is a key etiologic factor in DED pathophysiology.4 Although I do not test for elevated MMP-9, I believe that inflammation is likely present in any patient whose exam findings are consistent with visually significant DED.
Moreover, results from prospective studies analyzing the reliability of preoperative biometry data support the use of a medication that targets inflammation to treat DED prior to cataract surgery. For example, Kim et al reported improved accuracy of IOL power calculation in patients with DED treated for 14 days with a combination of loteprednol etabonate 0.5% and cyclosporine 0.05% compared with untreated controls.4 In 2 separate studies, Hovanesian et al found that treatment with lifitegrast ophthalmic solution 5.0% (Xiidra, Bausch + Lomb)) or cyclosporine ophthalmic solution 0.09% (Cequa, Sun Pharmaceuticals) for 28 days significantly improved the accuracy of preoperative biometry measurements used for IOL power calculations.5,6
Other clinical trial data showing that cyclosporine 0.09% is well-tolerated and fast acting make it a strong option for preoperative treatment of DED because these features favor treatment adherence and the likelihood that patients will be cleared for proceeding with surgery as scheduled when they return for repeat biometry after 3 weeks. Ratings of treatment comfort in pre-marketing clinical trials showed that 95% of patients using cyclosporine 0.09% experienced no worse than mild instillation pain.7 In the post-marketing COAT (Cequa Onset of Action Trial) study, patients using cyclosporine 0.09% twice daily showed significant improvements in higher order aberrations, corneal staining, TBUT, conjunctival redness, and symptoms as early as 1 week after starting treatment.8
In addition to controlling inflammation, my approach to managing DED in cataract surgery patients is tailored to the findings from both their history and clinical exam. Patients are counseled about modifiable environmental, behavioral, and systemic factors that can contribute to DED. Additional therapies are considered as needed, including cross-linked hyaluronic acid canalicular gel (Lacrifill, Nordic Pharma) to raise the tear film, perfluorohexyloctane ophthalmic solution (Miebo, Bausch + Lomb) for evaporative DED, acoltremon ophthalmic solution 0.003% (Tryptyr, Alcon Laboratories) twice a day for neurostimulation when there is more advanced DED, hypochlorous acid spray 0.01% (Avenova, EyePromise) for blepharitis, hypochlorous acid spray plus lotilaner ophthalmic solution 0.25% (Xdemvy, Tarsus Pharmaceuticals) for Demodex blepharitis, and omega supplements.
Conclusion
DED is often a chronic condition, so completion of the preoperative regimen does not mark the end of DED management for patients undergoing cataract surgery. By inciting inflammation and acting through several other mechanisms, cataract surgery can exacerbate preexisting DED, leading to bothersome symptoms and tear film instability that compromises quality of vision and causes patient dissatisfaction following cataract surgery. Ongoing management with medications for controlling inflammation, as well as other prescription therapies and in-office procedures, can help mitigate these risks and is important for preventing DED progression following cataract surgery.
Because cataract surgery can also induce DED, patients who did not require preoperative management should be informed about its potential development and the possibility of needing intervention. Setting proper patient expectations combined with detection and appropriate management of DED before and after cataract surgery are critical to maximizing postoperative satisfaction for all patients.
William B. Trattler, MD, is the Director of Cornea at the Center For Excellence in Eye Care in Miami, Florida, and focuses on cataract, corneal, and refractive surgeries.
Disclosures: Dr. Trattler is a consultant for Alcon Laboratories, Bausch + Lomb, Cassini Technologies, Johnson & Johnson, Oculus, Tarsus Pharmaceuticals, and Carl Zeiss Meditec.
References
- Trattler WB, Majmudar PA, Donnenfeld ED, McDonald MB, Stonecipher KG, Goldberg DF. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423-1430. doi:10.2147/OPTH.S120159
- Gupta PK, Drinkwater OJ, VanDusen KW, Brissette AR, Starr CE. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg. 2018;44(9):1090-1096. doi:10.1016/j.jcrs.2018.06.026
- Cochener B, Cassan A, Omiel L. Prevalence of meibomian gland dysfunction at the time of cataract surgery. J Cataract Refract Surg. 2018;44(2):144-148. doi:10.1016/j.jcrs.2017.10.050
- Kim J, Kim MK, Ha Y, Paik HJ, Kim DH. Improved accuracy of intraocular lens power calculation by preoperative management of dry eye disease. BMC Ophthalmol. 2021;21(1):364. doi:10.1186/s12886-021-02129-5
- Hovanesian J, Epitropoulos A, Donnenfeld ED, Holladay JT. The effect of lifitegrast on refractive accuracy and symptoms in dry eye patients undergoing cataract surgery. Clin Ophthalmol. 2020;14:2709-2716. doi:10.2147/OPTH.S264520
- Hovanesian JA, Berdy GJ, Epitropoulos A, Holladay JT. Effect of cyclosporine 0.09% treatment on accuracy of preoperative biometry and higher order aberrations in dry eye patients undergoing cataract surgery. Clin Ophthalmol. 2021;15:3679-3686. doi:10.2147/OPTH.S325659
- Cequa® (cyclosporine ophthalmic solution 0.09%). Sun Pharmaceutical Industries Inc. Accessed June 2, 2026. https://cequapro.com
- Hovanesian J, Berdy G, Sorensen R. CEQUA’s onset of action trial: an investigation of cyclosporine 0.09% speed of onset in improving ocular surface health in dry eye patients. Presented at the American Society of Cataract and Refractive Surgery Annual Meeting, April 25-28, 2025; Los Angeles.
Related Content