Emerging therapies and treatment for rare retinal diseases: a look at the pipeline
By John Wells, III, MD
The contents of this article are informational only and are not intended to be a substitute for professional medical advice, diagnosis, or treatment recommendations. This editorial presents the views and experiences of the author and does not reflect the opinions or recommendations of the publisher of Ophthalmology 360.
The management of patients with rare retinal diseases can pose a significant challenge to clinicians, particularly in the absence of approved therapies. It can be very difficult to face a patient and tell them that there is no treatment for what is causing their vision problems; however, lack of an approved treatment does not mean there is no hope. New therapeutic approaches for a variety of rare retinal diseases are currently being developed, and even now, we can take steps to mitigate complications and help patients gain a greater understanding of their condition.
X-Linked Retinitis Pigmentosa (XLRP)
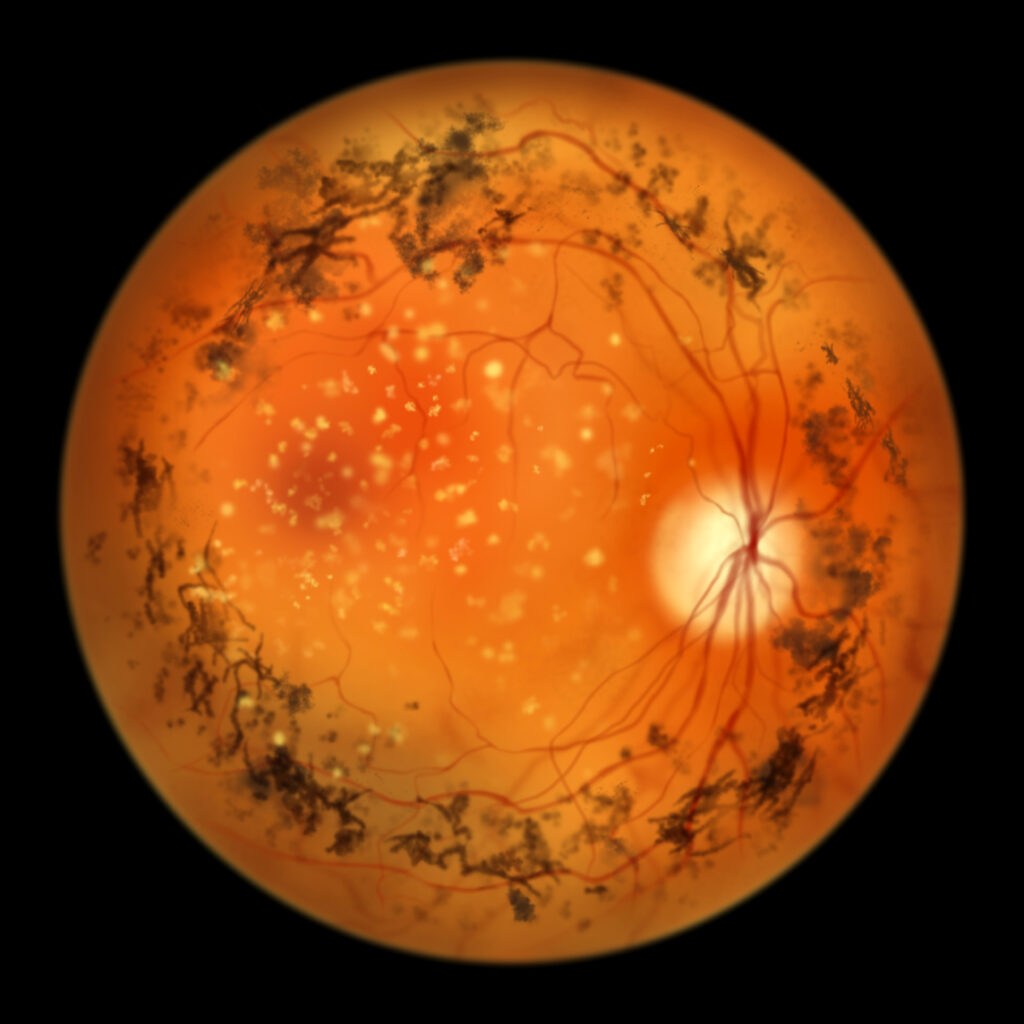
XLRP is a rare inherited retinal disease and is among the most severe forms of retinitis pigmentosa (RP). In XLRP, mutations in the RPGR gene lead to dysfunction in the metabolism of cone and rod cells, which, in turn, causes retinal degeneration.1
In the absence of an approved treatment for XLRP, we have patients come in on an annual basis to check for retinal pigment epithelium (RPE) loss with fundus autofluorescence; perform visual field testing; determine if they are developing cataracts; and use optical coherence tomography (OCT) to check for the development of cystoid macular edema (CME).
If a patient does develop cataracts, surgery can offer them significant visual benefits, but pre- and postoperative considerations must be carefully attended to, as patients with RP are at a higher risk for surgical complications.2 If a patient develops CME, carbonic anhydrase inhibitors (CAIs) such as oral acetazolamide or topical dorzolamide should be employed as first-line therapies. In patients intolerant of or unresponsive to CAIs, intravitreal or oral corticosteroids and intravitreal anti-vascular endothelial growth factor (VEGF) agents have also shown efficacy as second-line therapies.3
While there are no approved treatments for XLRP to date, a variety of gene therapy approaches are currently being pursued, which have demonstrated some efficacy in improving both visual field outcomes and some of the processes underlying XLRP-associated dysfunction in affected patients.4,5
Stargardt Disease
Stargardt disease is an autosomal recessive macular dystrophy in which patients, typically in their teens or early twenties, present with bilateral central visual loss and central scotomata. In Stargardt disease, mutations in the ABCA4 gene can lead to toxic levels of bisretinoid A2PE buildup in the photoreceptor membrane, causing RPE dysfunction and death.6
Diagnosis of Stargardt disease is usually done through observation of its characteristic appearance in the retina—in patients with Stargardt disease, the macula takes on a “beaten metal” like appearance with pisciform, or fish-shaped, flecks of lipofuscin surrounding the atrophic central macula. Stargardt disease can also be diagnosed by the identification of a dark choroid on fluorescein angiography, and autofluorescence or OCT imaging can be used to both diagnose Stargardt disease and track the progression of central atrophy.7
Stargardt disease is an area of active clinical investigation. In one approach, human embryonic stem cell-derived RPE cells were transplanted to protect photoreceptor cells and retinal function. While this approach was found to be safe for patients, no significant benefit to retinal function at 12 months following transplantation was observed.8
Gene therapy approaches have also been investigated for Stargardt disease, but a major limitation of these efforts is that the ABCA4 gene is too large for the adeno-associated virus (AAV) vectors that are commonly used in gene therapies.6 Studies have investigated the use of a lentivirus vector for gene therapy, and while one such study was terminated before completion for non-safety reasons, there is an ongoing follow-up study that is scheduled to be completed in 2033.9
Other approaches being investigated for the treatment of Stargardt disease are drugs that target different aspects of the retinoid cycle, either by lowering the formation of toxic byproducts or directly targeting toxic metabolites or pathways activated by these metabolites, like the complement cascade. Many of these studies are still ongoing, and it will be interesting to see if they demonstrate efficacy in improving visual outcomes in patients with Stargardt disease.9
Macular telangiectasia (MacTel) Type 2
MacTel type 2 is a progressive, bilateral, neurodegenerative disease in which Müller cells, which are glial cells that surround and provide nourishment to retinal neurons, become dysfunctional, leading to neuronal atrophy and disorganization of the outer retina. Over time, this causes significant difficulties with near vision and central visual field defects.10
Although it is considered a rare disease, MacTel type 2 is more common than was once thought.11 In my practice I frequently have patients referred for unexplained vision loss or blurring with an apparently normal exam, which turns out to be caused by MacTel type 2.
Diagnosis of MacTel can often be done clinically by observing its classic signs: gray opacification of the parafoveal macula, typically on the temporal side, but which can spread to involve the entire fovea; right angle venules; and sometimes the presence of small crystals in the retina. However, in early stages of the disease, most patients may still have good vision and the retina may appear mostly normal. In these cases, the use of OCT can be invaluable to identify signs of MacTel type 2 such as loss of Müller cells, loss of the outer nuclear layer and the ellipsoid zone (EZ), and the presence of degenerative cavities in the parafoveal retina.12
In later stages, patients with MacTel type 2 may develop subretinal neovascularization, known as proliferative MacTel, which can significantly threaten vision. Anti-VEGF agents have shown efficacy in treating this subretinal neovascularization but have not demonstrated efficacy in non-proliferative MacTel and do not treat its underlying causes.10
While there are currently no approved treatments for MacTel type 2, there are some exciting potential therapies on the horizon. Of particular note is NT-501, a surgically implanted encapsulated cell therapy (ECT) that delivers ciliary neurotrophic factor (CNTF), which acts as a neuroprotective agent for photoreceptors, into the vitreous cavity. NT-501 was found to be generally well tolerated in a phase 1 trial, and the results of phase 2 and 3 clinical trials demonstrated it slowed the progression of retinal degeneration, as measured by EZ loss and loss of retinal sensitivity.13,14 NT-501 is currently under review by the U.S. Food and Drug Administration and, if approved, would be the first therapy for MacTel type 2.
Another potential therapy for MacTel type 2 may be serine supplements, as serine deficits have been identified in patients with MacTel type 2. There is a phase 2 trial underway studying this approach, but data have yet to be published.15 See TABLE below for a snapshot of the therapies previously described.

Conclusion
Although gaps remain, the emergence of several new potential therapies for previously untreatable conditions offers hope to our patients with rare retinal diseases and makes it an exciting time to practice in the ophthalmic space. I look forward to seeing how the clinical trials and approvals for these conditions continue to evolve over time, and I eagerly anticipate a day when no retinal disease is considered untreatable.
John A. Wells, III, MD, is a retina and vitreous disease specialist practicing at Palmetto Retina Center in Columbia, SC. He is a consultant and has served on advisory boards for Genentech/Roche, 4DMT, Neurotech, and Ocular Therapeutix. He has also served as an investigator for Adverum, Astellas/Iveric, Aviceda, Eyebiotech, Eyepoint, 4DMT, Genentech/Roche, Kalaris, Kodiak, Lowy Medical Research Institute, Neurotech, Ocular Therapeutix, Oculis, Opthea, Outlook Therapeutics, and Regeneron/Bayer.
References
- MacLaren RE, Duncan JL, Fischer MD, et al. XOLARIS: a 24-month, prospective, natural history study of 201 participants with retinitis pigmentosa GTPase regulator-associated X-linked retinitis pigmentosa. Ophthalmol Sci. 2024;5(1):100595. doi:10.1016/j.xops.2024.100595
- Karti O, Saatci AO. Cataract surgery in retinitis pigmentosa. Med Hypothesis Discov Innov Ophthalmol. 2024;13(2):96-103. doi:10.51329/mehdiophthal1500
- Bakthavatchalam M, Lai FHP, Rong SS, Ng DS, Brelen ME. Treatment of cystoid macular edema secondary to retinitis pigmentosa: a systematic review. Surv Ophthalmol. 2018;63(3):329-339. doi:10.1016/j.survophthal.2017.09.009
- Cehajic-Kapetanovic J, Xue K, Martinez-Fernandez de la Camara C, et al. Initial results from a first-in-human gene therapy trial on X-linked retinitis pigmentosa caused by mutations in RPGR. Nat Med. 2020;26(3):354-359. doi:10.1038/s41591-020-0763-1
- Sladen PE, Naeem A, Adefila-Ideozu T, et al. AAV-RPGR gene therapy rescues opsin mislocalisation in a human retinal organoid model of RPGR-associated X-linked retinitis pigmentosa. Int J Mol Sci. 2024;25(3):1839. doi:10.3390/ijms25031839
- Tanna P, Strauss RW, Fujinami K, Michaelides M. Stargardt disease: clinical features, molecular genetics, animal models and therapeutic options. Br J Ophthalmol. 2017;101(1):25-30. doi:10.1136/bjophthalmol-2016-308823
- Kohli P, Tripathy K, Kaur K. Stargardt disease. In: StatPearls. Treasure Island (FL): StatPearls Publishing; January 8, 2024.
- Mehat MS, Sundaram V, Ripamonti C, et al. Transplantation of human embryonic stem cell-derived retinal pigment epithelial cells in macular degeneration. Ophthalmology. 2018;125(11):1765-1775. doi:10.1016/j.ophtha.2018.04.037
- Fujinami K, Waheed N, Laich Y, et al. Stargardt macular dystrophy and therapeutic approaches. Br J Ophthalmol. 2024;108(4):495-505. doi:10.1136/bjo-2022-323071
- Kedarisetti KC, Narayanan R, Stewart MW, Reddy Gurram N, Khanani AM. Macular telangiectasia type 2: a comprehensive review. Clin Ophthalmol. 2022;16:3297-3309. doi:10.2147/OPTH.S373538
- Klein R, Blodi BA, Meuer SM, Myers CE, Chew EY, Klein BE. The prevalence of macular telangiectasia type 2 in the Beaver Dam eye study. Am J Ophthalmol. 2010;150(1):55-62.e2. doi:10.1016/j.ajo.2010.02.013
- Chew EY, Peto T, Clemons TE, et al. Macular telangiectasia type 2: a classification system using multimodal imaging MacTel Project Report Number 10. Ophthalmol Sci. 2022;3(2):100261. doi:10.1016/j.xops.2022.100261
- Chew EY, Clemons TE, Jaffe GJ, et al. Effect of ciliary neurotrophic factor on retinal neurodegeneration in patients with macular telangiectasia type 2: a randomized clinical trial. Ophthalmology. 2019;126(4):540-549. doi:10.1016/j.ophtha.2018.09.041
- DeFino, A. Macular telangiectasia cell therapy meets primary endpoints in phase 3 trials. Healio. January 18, 2024. Accessed November 13, 2024. https://www.healio.com/news/ophthalmology/20240118/macular-telangiectasia-cell-therapy-meets-primary-endpoint-in-phase-3-trial
- MacTel SAFE Study. Lowy Medical Research Institute. March 4, 2024. Accessed November 13, 2024. https://www.lmri.net/mactel-safe-study/
Related Content