By Vinit Mahajan, MD, PhD
Introduction to Stargardt disease
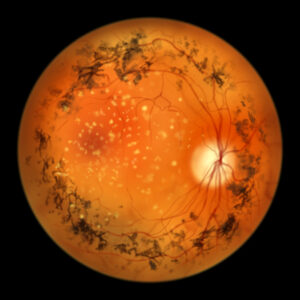
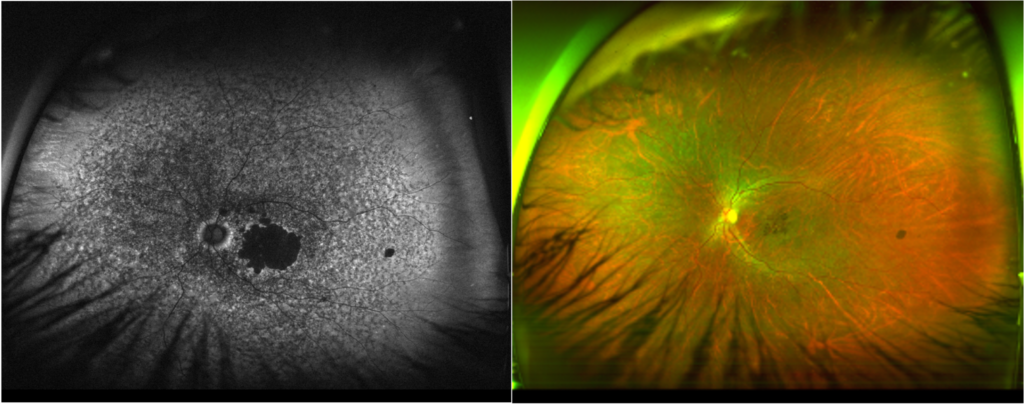
Stargardt disease is the most common form of inherited retinal disease (IRD)-related macular degeneration, affecting approximately 1 in 8,000 individuals worldwide.1,2 As the disease impacts the macula, the area of the retina responsible for sharp central vision, individuals with Stargardt disease have difficulty accomplishing everyday tasks such as reading, driving, and recognizing faces. This disorder is often diagnosed during childhood, though symptoms can manifest in adulthood.1,3
Stargardt disease is primarily linked to mutations in the ABCA4 gene. It is typically an autosomal recessive disease, meaning individuals who suffer from it possess 2 mutant copies of the ABCA4 gene, 1 inherited from each parent. People with 1 mutant copy of the gene are “carriers” and do not experience disease phenotypes. A child whose parents are carriers has a 25% chance of inheriting both disease copies.2
ABCA4 encodes for a protein of the same name that is responsible for transporting vitamin A in the visual cycle, the process in the retina that converts light into the electrochemical signals we perceive as vision.4 Defective ABCA4 leads to the toxic accumulation of vitamin A byproducts and cell debris, known as lipofuscin, within the retinal pigment epithelial cells and contributes to progressive macular degeneration and vision loss.1 There is currently no approved treatment for Stargardt disease.
Optogenetics: a new frontier
Optogenetics is a cutting-edge, promising therapeutic approach for treating retinal degenerative diseases like Stargardt disease. This approach involves the use of opsins, light-sensitive proteins, to render non-photoreceptor cells responsive to light. Opsins permit the flow of ions across the cell membrane upon light activation, which, in neurons, leads to changes in membrane potential and neuronal firing. By introducing opsins into retinal cells, typically through virally delivered gene therapy, optogenetics aims to restore vision by allowing these cells to respond to light. This approach could bypass damaged photoreceptors in the retina and restore vision in individuals with IRDs, offering hope for improved quality of life and vision outcomes.
MCO-010: a promising optogenetic therapy
MCO-010, a mutation-agnostic optogenetic therapy (Nanoscope Therapeutics) aims to address severe vision loss in patients with IRDs such as Stargardt disease and retinitis pigmentosa.5 MCO-010 induces the expression of multi-characteristic opsin (MCO) proteins specifically within the bipolar cells of the retina, which are located downstream of the damaged photoreceptors. MCO, a bioengineered highly-sensitive opsin protein, possesses broadband spectral responsiveness and fast kinetics, enabling activation of MCO-expressing bipolar cells even in ambient light conditions.5 The randomized, controlled RESTORE trial recently demonstrated the ability of MCO-010 to improve vision in patients with retinitis pigmentosa.
MCO therapy has also been evaluated in the phase 2 STARLIGHT study in patients with Stargardt disease. Enrollment criteria included a clinical or genetic diagnosis of Stargardt disease, as well as a best-corrected visual acuity (BCVA) between 1.3 logMAR (Snellen equivalent 20/400) and 1.9 logMAR (Snellen equivalent 20/1600) in the study eye and no better than 1.0 logMAR (Snellen equivalent 20/200) in the other eye. Patients were excluded if they had previously undergone gene or stem cell therapy. Three of the 6 enrolled patients presented with classic fleck macular degeneration phenotype.
Baseline measurements of BCVA using Early Treatment Diabetic Retinopathy Study (ETDRS) charts, visual field perimetry, and patient-reported outcomes using the Rasch-validated Michigan Retinal Degeneration Questionnaire (MRDQ) were recorded prior to intravitreal injection of MCO-010 in the study eye. BCVA measurements were assessed with and without a wearable magnifier. Patients were followed through week 48. An oral steroid prophylaxis tapering regimen was administered daily from day –3 to 17; a topical steroid eye drop regimen was administered daily from week 2 to 36.
Clinical trial outcomes and efficacy
Throughout the 48-week study, MCO-010 was efficacious. STARLIGHT patients showed a mean improvement of 5.5 ETDRS letters in BCVA 48 weeks after MCO-010 treatment, which reached an established benchmark from previous clinical trials.1 When BCVA was measured with the wearable magnifier at baseline and post-injection time points, the improvements were enhanced (13 ETDRS letters). Additionally, there was a 2.63 dB mean improvement in mean defect measured by visual field perimetry.
Patients also reported improvements in key MRDQ domain scores: reading and color and contrast. The most significant improvements in visual acuity were observed in patients with a macular degeneration phenotype, with a mean improvement in BCVA of 12 ETDRS letters at 48 weeks. With the wearable magnifier, the mean letter score improvement increased to 32 ETDRS letters. This suggests that this treatment may be beneficial for other macular degeneration patients. Importantly, MCO-010 treatment was well tolerated, with no reported serious adverse events or adverse events of special interest related to intraocular inflammation, such as endophthalmitis, retinitis, retinal vasculitis, or hypotony, further strengthening its candidacy as a successful therapeutic for Stargardt disease.
Optogenetic therapies like MCO-010 may prove to be a milestone in treating IRDs. Because delivery of a healthy copy of ABCA4 gene is difficult due to its large size, previous therapeutic attempts involved pharmacological agents to mitigate disrupted molecular pathways such as the visual cycle in Stargardt disease. Methods like MCO-010 effectively bypass the need to rescue or replace damaged or lost photoreceptors, respectively. One could imagine a future in which different gene therapy approaches and pharmacological methods are used together to create combinatorial therapeutics that are far more effective than any of the components individually. As such, optogenetic approaches could greatly broaden the treatment landscape for retinal diseases, especially in a mutation-agnostic manner.
Though the results are promising, challenges remain in using viral-mediated optogenetics to treat retinal diseases. One critical factor is the effectiveness of viral vectors to deliver genes to the target cells. Current research aims to improve delivery to specific cell types by engineering the capsid of the viral vector.6 MCO-010 uses an engineered AAV vector to effectively transduce the inner retina upon single intravitreal injection. Selective MCO expression in the targeted ON-bipolar cells is achieved by a genomic element (mGluR6 promoter-enhancer). Finally, the sustained efficacy of current therapeutics remains to be seen. Liquid-biopsy proteomics has the potential to understand changes during disease progression and the health of target cells to enable optimal intervention.7 Long-term studies in patients will help shed light on the magnitude of the difference between the treated patients and the progressively degenerating disease population.
As we advance the next generation of therapeutics for retinal diseases, the field of ophthalmology must maintain a collaborative culture among scientists, clinicians, regulators, and patient advocacy groups. Basic and translational science continues to advance our understanding of the molecular and cellular mechanisms involved, while also creating patient-centric tools for effectively delivering light-sensitive opsin-encoding genes. Clinical trials like STARLIGHT and RESTORE evaluate the efficacy of these tools and identify the patient populations that will benefit the most. At the convergence of these efforts, we aim to discover groundbreaking methods to fulfill the unmet medical needs of the retinal disease community.
Vinit Mahajan, MD, PhD, is professor and vitreoretinal surgeon and scientist in the Department of Ophthalmology at Stanford University.
References
- Wang L, Shah SM, Mangwani-Mordani S, Gregori NZ. Updates on emerging interventions for autosomal recessive ABCA4-associated Stargardt disease. J Clin Med. 2023;12(19):6229. doi:10.3390/jcm12196229
- Coussa RG, Utz VM, Traboulsi EI. Stargardt disease (STGD). August 21, 2017. Accessed August 2, 2024. https://www.aao.org/education/disease-review/stargardt-disease-stgd
- Stargardt disease. Foundation Fighting Blindness. Accessed August 2, 2024. https://www.fightingblindness.org/diseases/stargardt-disease
- Tanna P, Strauss RW, Fujinami K, Michaelides M. Stargardt disease: clinical features, molecular genetics, animal models and therapeutic options. Br J Ophthalmol. 2017;101(1):25-30. doi:10.1136/bjophthalmol-2016-308823
- Batabyal S, Gajjeraman S, Pradhan S, et al. Sensitization of ON-bipolar cells with ambient light activatable multi-characteristic opsin rescues vision in mice. Gene Ther. 2021;28(3-4):162-176. doi:10.1038/s41434-020-00200-2
- De Silva SR, Moore AT. Optogenetic approaches to therapy for inherited retinal degenerations. J Physiol. 2022;600(21):4623-4632. doi: 10.3389/fnins.2020.570909
- Wolf J, Rasmussen DK, Sun YJ, et al. Liquid-biopsy proteomics combined with AI identifies cellular drivers of eye aging and disease in vivo. Cell. 2023;186(22):4868-4884. doi:10.1016/j.cell.2023.09.012
Related Content