Although visual acuity remains relatively stable over time in patients with X-linked retinoschisis (XLRS), the development of outer retinal loss and the presence of certain retinoschisin gene (RS1) genotypes are associated with poorer long-term visual outcomes, according to a study.
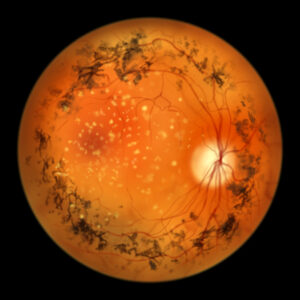
In this retrospective chart review, 52 patients with XLRS from 33 families with a median age of 5 years at symptom onset, with a median follow-up period of 5.7 years, were included. Macular retinoschisis, characterized by the separation of retinal layers, was observed in 99.0% of the 104 eyes studied. Peripheral retinoschisis occurred in 46.2% of the eyes, most frequently in the inferotemporal quadrant (40.4%).
The study found that the initial and final visual acuity (VA) measurements were comparable, indicating relatively stable vision over time. However, the analysis found that 92.6% of the eyes developed detectable outer retinal loss by age 20, and 43.9% exhibited focal or diffuse outer retinal atrophy (ORA) by age 40. The presence of ORA, but not central subfield thickness (CST), was associated with reduced VA.
Researchers noted a modest correlation between VA and CST across both eyes as well as a stronger association between VA and CST in the same eye. Carbonic anhydrase inhibitors (CAIs), commonly used to treat macular edema, were found to improve CST, but their effect on VA was not significant.
The study found that 7.7% of the eyes experienced XLRS-related retinal detachment (RD), which was associated with poorer visual outcomes compared to eyes without RD. Notably, patients with null RS1 genotypes had a higher likelihood of experiencing at least moderate visual impairment at final follow-up. This correlation remained significant even after accounting for age at onset, initial CST, initial ORA, or previous RD.
Reference
Fenner BJ, Russell JF, Drack AV, et al. Long-term functional and structural outcomes in X-linked retinoschisis: implications for clinical trials. Front Med (Lausanne). 2023;10:1204095. doi: 10.3389/fmed.2023.1204095. PMID: 37396901; PMCID: PMC10310546.
Related Content