A retina/uveitis specialist explores the latest thinking on and treatment patterns in intraocular inflammation
By Danny A. Mammo, MD
It is estimated that 10% of blindness in the United States is due to uncontrolled inflammation in uveitis and resulting complications.1 Managing the diverse conditions under this umbrella, many of which are idiopathic, is an important challenge for retina specialists, whether or not we choose to subspecialize in uveitis. In this article, I discuss my perspective as a recent vitreoretinal surgical fellow at Cole Eye Institute, Cleveland Clinic, around current thinking on the diagnosis and treatment of intraocular inflammation.
Being a Fellow Today
I think it is a wonderful time to be an ophthalmology resident or vitreoretinal fellow treating intraocular inflammation, for a few reasons. One is all the advances in diagnostic tools and treatments that we have available. Another is that ever since COVID, we have seen a widespread effort toward the development of virtual platforms that give residents and fellows experience with technologies, techniques, and/or unusual cases that they might not have access to at their own institutions. Given the ongoing changes in drug delivery systems and multimodal imaging tools, residents and fellows have more resources than ever to learn, so it’s an interesting time.
In the realm of uveitis, residents and fellows will gain facility with local clinic-based therapies, such as injecting Ozurdex (dexamethasone intravitreal implant, 0.7 mg), Yutiq (fluocinolone acetonide intravitreal implant, 0.18 mg), or the suprachoroidal Xipere (triamcinolone acetonide injectable suspension, 40 mg/mL), as well as surgical interventions, such as mastering implantation of Retisert (fluocinolone acetonide intravitreal implant, 0.59 mg) (Table 1). In addition, we learn how to effectively follow-up and handle the array of potential complications that may ensue from intra- and peri-ocular steroid therapies—all of which help increase our comfort as we transition to becoming attendings.
It is also important that we gain exposure to the kinds of assessments and treatments that may be administered to uveitis patients by rheumatologists, pulmonologists, and other co-managing physicians. Knowing about the range of biologics and other steroid-sparing systemic therapies, their mechanisms, and the most common side effects empowers us to provide the best possible management of these patients.
Managing Chronic Intraocular Inflammation: Diagnosis and Treatment
Challenges in the management of patients with uveitis begin at diagnosis, which is inherently difficult because of the substantial overlap in signs and symptoms between different infectious and inflammatory eye conditions. Diagnosing uveitis requires a careful, detailed workup, interpretation of laboratory tests, and, ideally, multimodal imaging.1 Today, the exam entails not only looking at the patient in front of us but also integrating a great deal of information from clinical images and testing. Understanding how to interpret all of this data efficiently but thoroughly is key to arriving at the diagnosis.
Although a single episode of anterior uveitis may not require a laboratory workup, recurrence should elicit further evaluation to rule out underlying autoimmune or infectious processes. Due to a higher risk of permanent vision loss and an association with systemic disease, additional analysis with a broad differential is necessary for intermediate, posterior, and panuveitis.1
The exam helps determine how aggressively to treat, and whether to use local and/or systemic therapies. Laboratory and ancillary imaging, such as computed tomography (CT) of the chest, help determine if a given presentation is predominantly local or systemic. I also consider the age of the patient and status of the lens—however, if systemic treatment is insufficient, associated with intolerable side effects, or even unfeasible due to insurance issues, age or lens status will not prevent me from using local treatment. Oftentimes, to achieve control of inflammation, a combination of local and systemic therapy is necessary.2 In some cases, the use of newer imaging modalities can make a difference in diagnostic accuracy.
Therapeutic and Technological Advances
One of the biggest recent technological advances in the field of retina is widefield imaging, which greatly helps with correctly diagnosing uveitis. Seeing more of the retina allows us to visualize diagnostic clues and even the presence of inflammation that could otherwise be missed.3-5 Although other advances, such as genetic testing and biomarkers discovered through ocular proteomics, may be exciting, widefield imaging remains the most tangible and available diagnostic innovation in uveitis.6,7
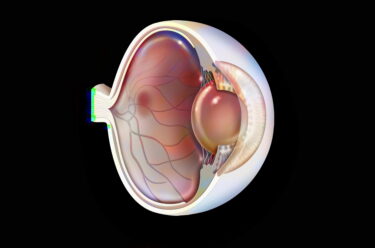
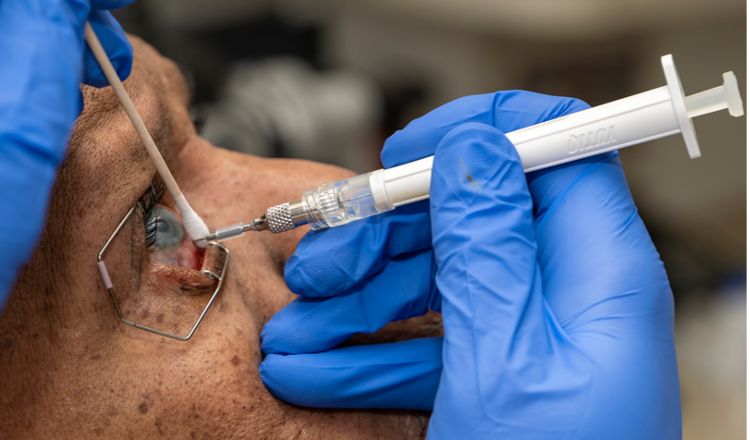
Therapeutically, there have been several changes in the past 10 to 15 years. Intravitreal drug delivery systems, such as Ozurdex and more recently, YUTIQ, have expanded our toolbox in dealing with difficult-to-control, chronic uveitic conditions (Figure 1). Suprachoroidal drug delivery (as in the case of Xipere) also shows promise; we can expect our understanding of its role in the treatment of uveitis and the nuances of the injection technique to evolve as its use becomes more widespread.8 And although Retisert is a more invasive and older intervention, it is still appropriate for many patients, so it’s important for residents and fellows to learn about both the implantation procedure itself and the best practices for management of postoperative complications.
New biologics and biosimilars are also always being developed. The most prescribed biologics for patients with non-infectious uveitis are anti-tumor necrosis factor-α antibody-based drugs, specifically, infliximab and adalimumab. These medications have biosimilar counterparts, although there is concern that biosimilars may lead to more relapse.9,10 In uveitis as elsewhere in retina, specialists increasingly need to be aware of data on available biosimilars and how their clinical evidence compares to that of reference biologic medications.
Looking Ahead
Currently under investigation for the treatment of uveitis are local and systemic formulations of biologics that may specifically target inflammatory markers without the side effects of steroids.11 One of these candidates is intravitreal sirolimus, which may provide benefits in patients with non-infectious uveitis for up to one year.11-13 Filgotinib, a Janus kinase inhibitor, was recently found in a randomized, controlled trial to reduce the risk of uveitis flare compared to placebo but safety issues about JAK inhibitors and their risk of thrombotic events and decreased sperm counts may limit their use in some high-risk patients.14,15 Izokibep blocks interleukin-17A, which plays a major role in the inflammatory cascade; a phase 2b pivotal study is currently recruiting in patients with active non-infectious uveitis requiring high-dose steroids.11,16 An interleukin-6 blocker, Tocilizumab, is also being investigated for non-infectious uveitic macular edema.17
I think the use of long-term intravitreal therapies, such as Yutiq, will become more common in the management of intraocular inflammation over the next 5 to 10 years. Looking further ahead, we still have a long way to go in deepening our understanding and our ability to apply individualized medicine in uveitis. We do know that in some forms of uveitis, based on a patient’s cytokine expression profile, particular protein networks, and molecular pathways may be altered. Hopefully, future advances in genetic testing, personalized proteomics, and identification of inflammatory markers will help us to provide more personalized and tailored treatment to control inflammation.18
In the end, it’s gratifying to be involved in the study of retina and uveitis and the care of these patients. When looking at the posterior segment and uveitic inflammatory conditions, our patients often have problems that affect multiple organ systems, where the eye may be the only symptomatic organ. We are privileged to be able to not only diagnose these conditions but also provide guidance to our colleagues in other specialties on what may be going on and offer insight into how best to treat our patients.

Danny A. Mammo, MD, is a vitreoretinal surgical and uveitis specialist at the Cole Eye Institute, Cleveland Clinic, Cleveland, OH.
References
- Duplechain A, Conrady CD, Patel BC, Baker S. Uveitis. National Library of Medicine. Updated May 24, 2022. Accessed August 4, 2022. https://www.ncbi.nlm.nih.gov/books/NBK540993/
- Mehta NS, Emami-Naeini P. A Review of systemic biologics and local immunosuppressive medications in uveitis. J Ophthalmic Vis Res. 2022;17(2):276-289.
- Charters L. Technologies offer options in treatment of uveitis. Ophthalmology Times. 2021;46(17).
- Marchese A, Agarwal A, Moretti AG, et al. Advances in imaging of uveitis. Ther Adv Ophthalmol. 2020;12:2515841420917781.
- Emami-Naeini P, Sharm S. Getting a good look at uveitis with multimodal imaging. Retina Today. September 2018. Accessed October 13, 2022. https://assets.bmctoday.net/retinatoday/pdfs/0918RT_Subfocus_Sharma_Index.pdf
- Cunningham ET Jr, Pichi F, Mahajan VB, Rosenbaum JT, Zierhut M. Genetics of uveitis. Ocul Immunol Inflamm. 2021;29(2):215-218.
- Bansal R, Gupta A. Protein biomarkers in uveitis. Front Immunol. 2020;11:610428.
- Deaner JD, Sharma S. Future therapies in uveitis. November 1, 2020. Accessed October 13, 2022. https://www.retinalphysician.com/issues/2020/november-december-2020/future-therapies-in-uveitis
- Ferreira LB, Smith AJ, Smith JR. Biologic drugs for the treatment of noninfectious uveitis. Asia Pac J Ophthalmol (Phila). 2021;10(1):63-73.
- Deaner JD, Srivastava SK, Hajj-Ali RA, et al. Recurrence rates of inflammation after switching from the originator infliximab to biosimilar infliximab-abda for noninfectious uveitis. Am J Ophthalmol. 2021;225:172-177.
- Arepalli S. Current trials in uveitis. October 1, 2022. Accessed October 13, 2022. https://www.retinalphysician.com/issues/2022/october-2022/current-clinical-trials-in-uveitis
- Ibrahim MA, Sepah YJ, Watters A, et al. One-year outcomes of the SAVE study: sirolimus as a therapeutic approach for uveitis. Transl Vis Sci Technol. 2015;4(2):4.
- Cabahug VLO, Uy HS, Yu-Keh E, Sapno KJD. Outcomes of treatment with sirolimus for non-infectious uveitis: a meta-analysis and systematic review. Clin Ophthalmol. 2019;13:649-669.
- Srivastava S, Watkins T, Nguyen QD, et al. A phase 2 randomized controlled trial of the Janus Kinase (JAK) inhibitor filgotinib in patients with noninfectious uveitis. Abstract presented at: ARVO Annual Meeting; May 1-4, 2022; Denver, CO and virtually.
- Summary of risk management plan for Jyseleca® (filgotinib). European Medicines Agency. Updated September 11, 2022. Accessed November 21, 2022. https://www.ema.europa.eu/en/documents/rmp-summary/jyseleca-epar-risk-management-plan-summary_en.pdf
- Phase 2b pivotal study of izokibep in non-infectious, intermediate-, posterior-, or pan-uveitis. ClinicalTrials.gov identifier: NCT05384249. https://clinicaltrials.gov/ct2/show/NCT05384249. Updated October 13, 2022. Accessed October 13, 2022.
- Karkhur S, Hasanreisoglu M, Vigil E, et al. Interleukin-6 inhibition in the management of non-infectious uveitis and beyond. J Ophthalmic Inflamm Infect. 2019;9(1):17.
- Velez G, Roybal CN, Colgan D, Tsang SH, Bassuk AG, Mahajan VB. Precision medicine: personalized proteomics for the diagnosis and treatment of idiopathic inflammatory disease. JAMA Ophthalmol. 2016;134(4):444-8.
- Mishra K, Leng T.Steroid therapy for the long haul. Retina Today. January/February 2022. Accessed October 31, 2022. https://retinatoday.com/articles/2022-jan-feb/steroid-therapy-for-the-long-haul
- Thorne JE, Sugar EA, Holbrook JT, et al. Periocular triamcinolone vs. intravitreal triamcinolone vs. intravitreal dexamethasone implant for the treatment of uveitic macular edema: the periocular vs. intravitreal corticosteroids for uveitic macular edema (POINT) trial. Ophthalmology. 2019;126(2):283-295.
- Khurana RN, Merrill P, Yeh S, et al. Extension study of the safety and efficacy of CLS-TA for treatment of macular oedema associated with non-infectious uveitis (MAGNOLIA). Br J Ophthalmol. 2022;106(8):1139-1144.
- Campochiaro PA, Brown DM, Pearson A, et al. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology. 2011;118(4):626-635.e2.
- Jaffe GJ, Pavesio CE; Study Investigators. Effect of a fluocinolone acetonide insert on recurrence rates in noninfectious intermediate, posterior, or panuveitis: three-year results. Ophthalmology. 2020;127(10):1395-1404.
Related Content