
By Kambiz Silani, OD
In our dry eye clinic, we offer multifaceted therapy, relying heavily on the latest in-office procedures (Intense Pulsed Light [IPL], thermal pulsation, eyelid debridement, gland probing and amniotic membrane), complemented by medications, supplements, and at-home care. We also recommend lubricating eye drops that combine 2 key ingredients: hyaluronic acid (HA) and trehalose for symptom relief.
Studies of HA + Trehalose
For years, we’ve been using drops with HA, a water-loving molecule that retains moisture to help lubricate and protect the corneal epithelium. Trehalose is somewhat of a newcomer in the United States. It is a bioprotectant that fortifies the cells on the ocular surface, so they do not suffer as much damage from dryness. Studies show that HA and trehalose work better together, compared to drops with HA alone.1-5
Eye drops with HA and trehalose significantly increase tear film thickness for up to 240 minutes from a single use, compared to up to 40 minutes with drops that contain HA alone.1 The combination is significantly better than HA alone in improving patients’ ocular surface disease index (OSDI), even for severe dry eye.2 The combination also improves tear breakup time (TBUT) and staining;3 decreases inflammation, stinging, and itching;4 and is more effective against dry eye than artificial tears for cataract surgery patients.5
I’ve been recommending iVIZIA (Thea), a combination of 3% trehalose, 0.15% HA, and viscosity-boosting povidone, as well as Optase MGD (Scope) to my patients. I’ve also personally used iVIZIA.
My patients tell me they feel the effects very quickly, and their eyes feel better for a longer duration, compared to lubricating drops they were using before. iVIZIA drops are preservative-free, so we’re also eliminating preservatives that can exacerbate dry eye. The difference is night and day for patients who have been using preserved drops, particularly if they contain BAK or a vasoconstrictor. We also continue to recommend HA drops without trehalose, such as Oasis Tears (Oasis), Optase Dry Eye Intense PF (Scope), and Systane Hydration PF (Alcon).
Patient Case Studies
Everyone needs a lubricating drop, so I recommend these drops to patients of all ages with mild to severe dry eye disease, including contact lens wearers. Patients particularly appreciate them when they need an extra boost after a long day in contact lenses, between in-office treatments, and in dry travel environments (particularly around blowing vents in cars, trains, and airplanes).
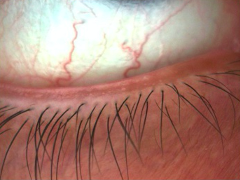
Frequent traveler: A 38-year-old male patient with mild to moderate dry eye disease secondary to meibomian gland dysfunction (MGD) traveled for work often. He experienced intermittent and bothersome ocular symptoms of burning, itching, and foreign body sensation, especially when flying or reading for prolonged periods. His abnormal SPEED score was 21/28, and he emphasized that his condition really interfered with his quality of life. During the consult, his TBUT was nearly 2 seconds, and he had mild punctate keratitis, mild papillae, significant structural changes to his meibomian glands, normal tear meniscus height (TMH), and mild conjunctival redness. (Figure 1)
The patient underwent OptiLight, with exceptional results. I instructed him to take high-quality omega-3 supplements (DE 3, PRN), use preservative-free allergy eye drops for ocular allergies, and use iVIZIA eye drops while traveling to improve his comfort. Three months later, his SPEED score was significantly improved to 8/28, his keratitis resolved, and his TBUT increased to 7 seconds. Mostly importantly, he shared that his symptoms were well controlled.
Severe dry eye: A 67-year-old woman had a history of severe dry eye disease, ocular rosacea, filamentary keratitis, nocturnal lagophthalmos, and MGD for many years. At her initial visit, her SPEED score was at its peak of 28/28. Her condition’s severity led her to multiple dry eye specialists without much relief, so she took a leave of absence from work. During her workup, her TMH was normal, her TBUT was moderately reduced, her conjunctival redness was severe, she had major loss of meibomian gland structures, and there was significant eyelid telangiectasia. With vital dye staining, she had a reduced TBUT of approximately 5 seconds, moderate lid wiper epitheliopathy (LWE), moderate punctate keratitis, as well as filaments on her ocular surface. (Figure 2)
Thankfully, the patient responded favorably to office-based treatment including OptiLight, LipiFlow, Prokera (BioTissue), and BlephEx. For her home routine, we started her on RegenerEyes Pro, iTear 100 neuro-stimulation (Olympic Ophthalmics), autologous serum tears, Mucomyst (UPSA), Optase Hylo Night nighttime ointment (Scope), and iVIZIA drops for relief between her in-office treatment visits. With this proactive and multi-faceted approach, the patient slowly returned to work, her keratitis and filaments resolved, and her SPEED score improved to 16/28.
Contact lens wearer: A 31-year-old woman had moderate dry eye disease in both eyes, which led to contact lens intolerance, fluctuating vision, and eye fatigue. At her initial visit, she had been suffering for about 5 months. She had an abnormal SPEED score of 16/28. During her evaluation, it was determined that she had reduced TBUT (evaporative dry eye) with mild punctate keratitis and LWE.
With the help of IPL (OptiLight, Lumenis), thermal pulsation (LipiFlow, Johnson & Johnson Vision), and eyelid debridement (BlephEx, Alcon), her SPEED score dropped to 2/28, her keratitis resolved, and her tear film stabilized. Additionally, I started her on Regener-Eyes Lite (Regener-Eyes) biologic eye drops and iVIZIA lubricating drops, which allowed her to comfortably wear her contact lenses all day.
It’s always exciting when we can help patients through a multifaceted approach. Lubricating drops with HA and trehalose contribute to that goal while letting us bring patients something new that works significantly better than what we used in the past. And because patients are familiar with using lubricating drops, they notice the difference, which adds to their perception of the care they receive at our dry eye clinic.
References
- Schmidl D, Schmetterer L, Witkowska KJ, et al. Tear film thickness after treatment with artificial tears in patients with moderate dry eye disease. Cornea. 2015;34(4):421-426.
- Fondi K, Wozniak PA, Schmidl D, et al. Effect of Hyaluronic Acid/Trehalose in Two Different Formulations on Signs and Symptoms in Patients with Moderate to Severe Dry Eye Disease. J Ophthalmol. 2018;2018:4691417.
- Fondi D, Wozniak PA, Schmidl D, et al. Effect of Hyaluronic Acid/Trehalose in Two Different Formulations on Signs and Symptoms in Patients with Moderate to Severe Dry Eye Disease. J Ophthalmol. 2018;2018:4691417.
- Chiambaretta F, Doan S, Labetoulle M, et al. A randomized, controlled study of the efficacy and safety of a new eyedrop formulation for moderate to severe dry eye syndrome. Eur J Ophthalmol. 2017;27(1):1-9.
- Mencucci R, Favuzza E, Decandia G, et al. Hyaluronic Acid/Trehalose Ophthalmic Solution in Reducing Post-Cataract Surgery Dry Eye Signs and Symptoms: A Prospective, Interventional, Randomized, Open-Label Study. J Clin Med. 2021;10(20):4699.
Kambiz Silani, OD, is the Chief Clinical Director of Beverly Hills Optometry. In 2013, he founded the practice’s Advanced Dry Eye Center in Beverly Hills, California (www.bheyeguy.com).
Related Content





